Again, this is a quick sketch to raise some questions, so forgive the accuracy…
These questions could apply to any pathway and any Acute Trust, but I’m starting with Cancer.
- I want to know more about what happens in hospital once you are referred?
- I suspect that too much depends on bits of paper or disconnected systems.
- I suspect the system is not how the staff or patients would like it.
- How can we help?





Some of this is happening, some on the way, some I am unclear on, but I believe needs improving.
- How do we systematically look at every step of the pathways, and understand what would be helped by better systems.
- How do we empower patients and carers to track their appointments and not miss important ones, and to have the information and support that they need. This issue is more a feature of non-cancer pathways, but I have patients regularly tell me that they have been informed that they Did Not Attend (DNA’d) an appointment that they did not know about. This is a waste for everyone. I understand that the appointments system is being/has been improved, so hopefully more detail to follow soon.
- How are we improving the intelligence of the system, eg. How do we know how much capacity we need and where the bottlenecks are? How do we track patients, diagnostics or histology samples? How do we get the diagnostics results safely and electronically to the requesting clinicians, and how timely and safe is this?
With the help of colleagues and patients, I would like to add more detail to the above picture soon…
UPDATE 30.10.16: Rough sketch of just some of the opportunities to improve care. Where better processes, I.T. & citizens/people/patients/carers can help and where paper needs to move to electronic.

Just a few ideas (below) where we could improve (with contributons from Jason and Manas, especially the idea of offering SCRAI to patients at the point of referral).
I know some of the ideas below are underway, but may need some support. I know there’s a lot I have not mentioned and this needs describing.
The NHS is based on treating need, so this is an opportunity for (and needs to be done in a way, that allows) those more able and the system, to help those less able and with more need (while supporting themselves and the system).
Also there is much treacle to get through to share information between parts of the NHS & Social Care. If we give it to the patients (while we continue to improve the relevant NHS/Social Care interoperabilty) they will arrive at their appointments better informed with mor tools at their disposal.

We are working on the GP referral letter and Hospital communications. We know that improved clarity especially on Urgency, Specialty, reason for referral help the patient and the system. We know there’s great variablity in Hospital letters.
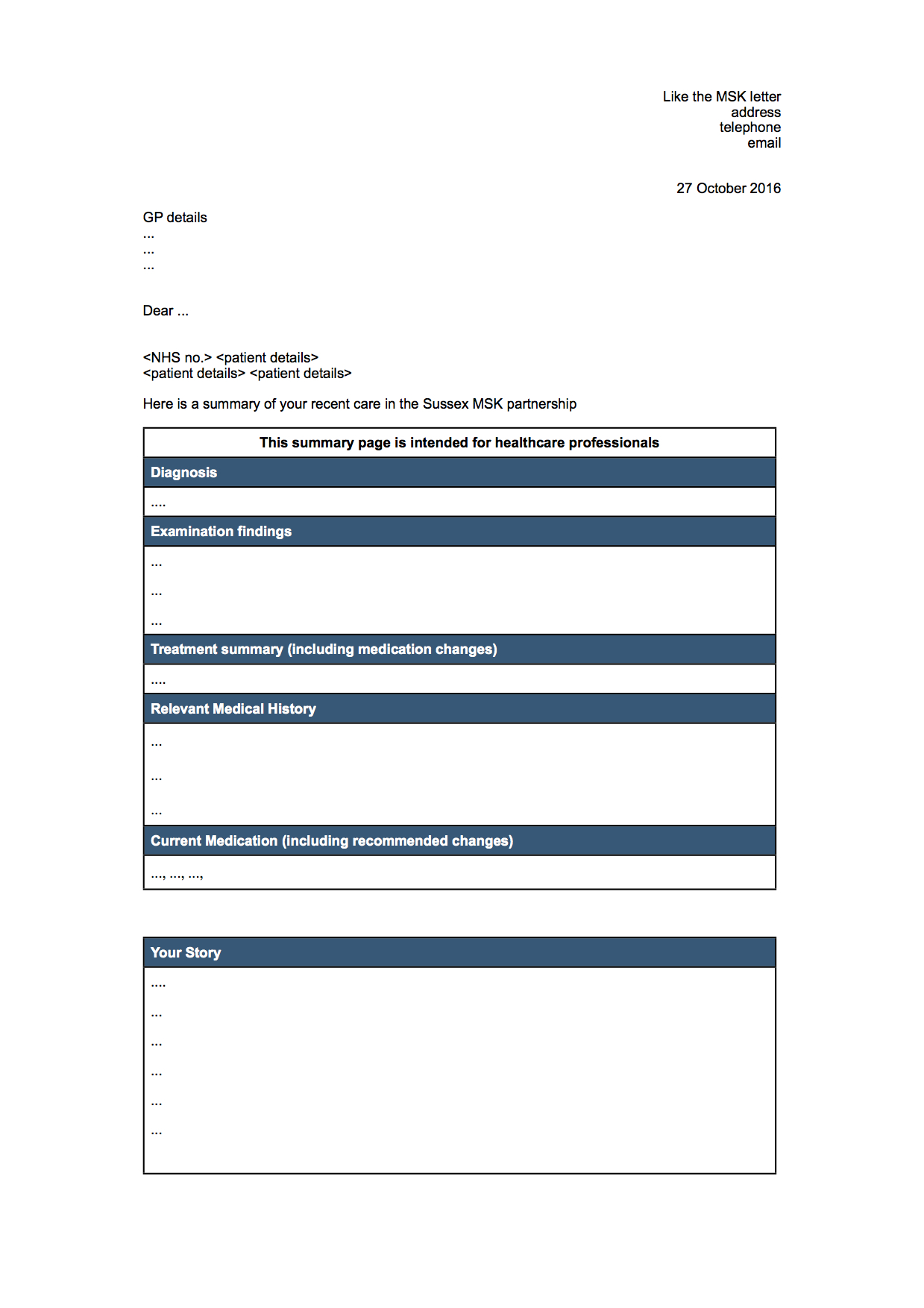
Also making best use of the systems, where accurate information is recorded, this can be used to create more accurate letters. The coloured text in the drafts below, will disappear as these are tags for the data to auto-populate from the GP system.
DRAFT GP Referral minimum dataset:

DRAFT Out-patient letter template:
I am keen to extend the use of patient portals/PHRs (patient held records).
Some seem more Primary/Community care and others more Secondary Care oriented.
I am sure each has their particular use and benefit.
The Digitial NHS site has some useful information, so worth a read. The Digital Primary Care page has the 2016-18 GPIT operating model, p145 Appendix 4 Digital Maturity Assessment ref 100 “Patients can record their personal health data which is accessible online by the GP. Patients and GPs can online, collaboratively set goals and care outcomes and track progress against these”.
The Nuffield report “Digital requirements for new primary care models” also mentions patient tools.